|
This article may be reprinted free of charge provided 1) that there is clear attribution to the Orthomolecular Medicine News Service, and 2) that both the OMNS free subscription link http://orthomolecular.org/subscribe.html and also the OMNS archive link http://orthomolecular.org/resources/omns/index.shtml are included. |
|
|
FOR IMMEDIATE RELEASE HOW WE CAN FIX THIS PANDEMIC IN A MONTHCommentary by Damien Downing, MBBS, MRSB(OMNS June 22, 2020) If we act on the data showing that it is highly probable that vitamin D can save lives, we could fix this pandemic in a month, for perhaps $2 per person. There would be no significant adverse effects. If we wait for "evidence" that vitamin D mitigates the impact of COVID-19, thousands more will die. If we could arrange to give everyone vitamin D, and it failed to protect them, so what? The risk from not acting is much greater than the risk from acting. Dosage is important and generally misunderstood. Two countries have acted on this already: Egypt and Slovenia. Why can't we? The Orthomolecular Medicine News Service has been publicizing the importance of vitamins D and C, and the minerals zinc and magnesium, in this pandemic since January [1]. I have been writing about Vitamin D and sunlight for over 30 years [2], and it has never been more relevant. If you caught the COVID19 virus right now, having a good vitamin D status (from already having taken a supplement) would
This is not "proven" or "evidence-based" until we have done controlled trials comparing it to placebo. Any volunteers for that? But the data, already strong, has been pouring in since the start of the pandemic. Here's the data for the two statements above. [A Hazard Ratio of 4 means that in one condition, for instance vitamin D deficiency, you are 4 times more likely to suffer the "hazard" than in another condition, say vitamin D adequacy. The graphics are all mine.] A Philippine study [3]With a deficient vitamin D status (<50nmol/L) the probability of becoming Severe or Critical with COVID-19 was 72.8% against 7.2% with adequate vitamin D (>75nmol/L). The Hazard Ratio is 10.0. 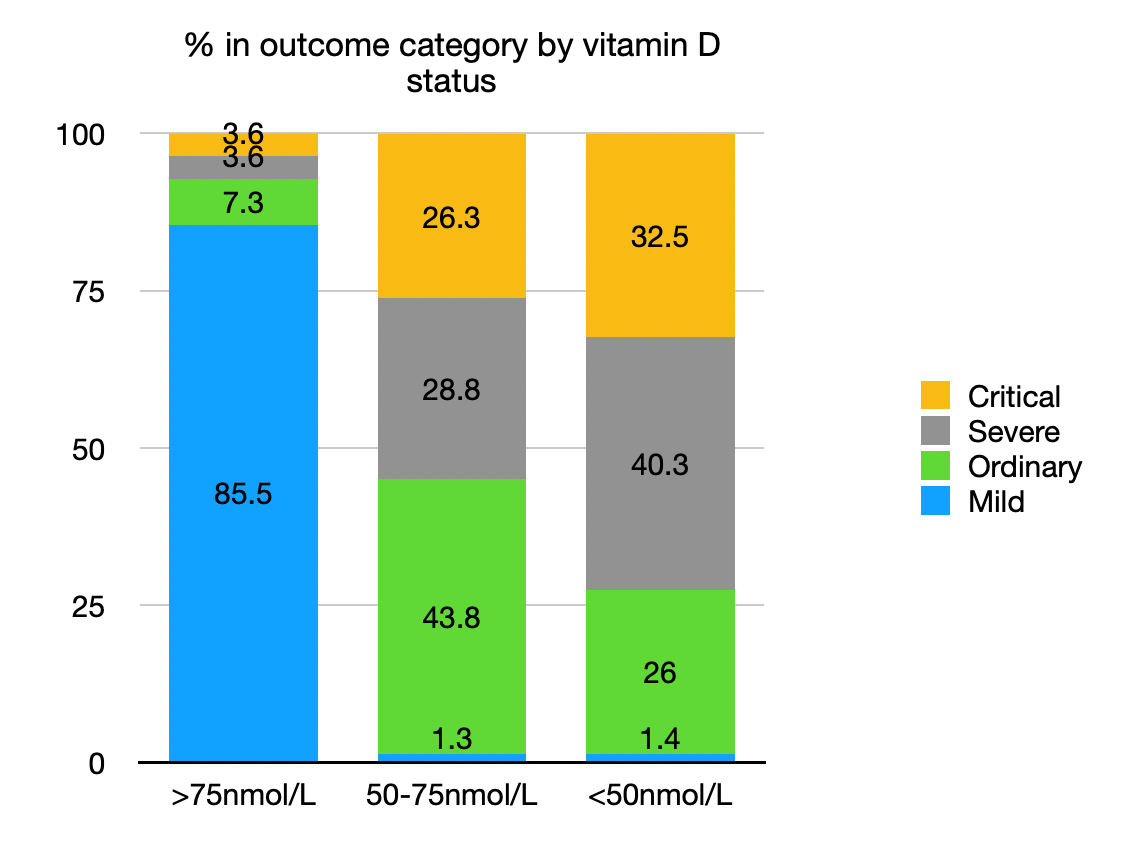 An Indonesian study [4]With a deficient vitamin D status (<50nmol/L) the mortality rate from COVID-19 was 98.8% against 4.1% with adequate vitamin D (>75nmol/L). The Hazard Ratio is 24.1. 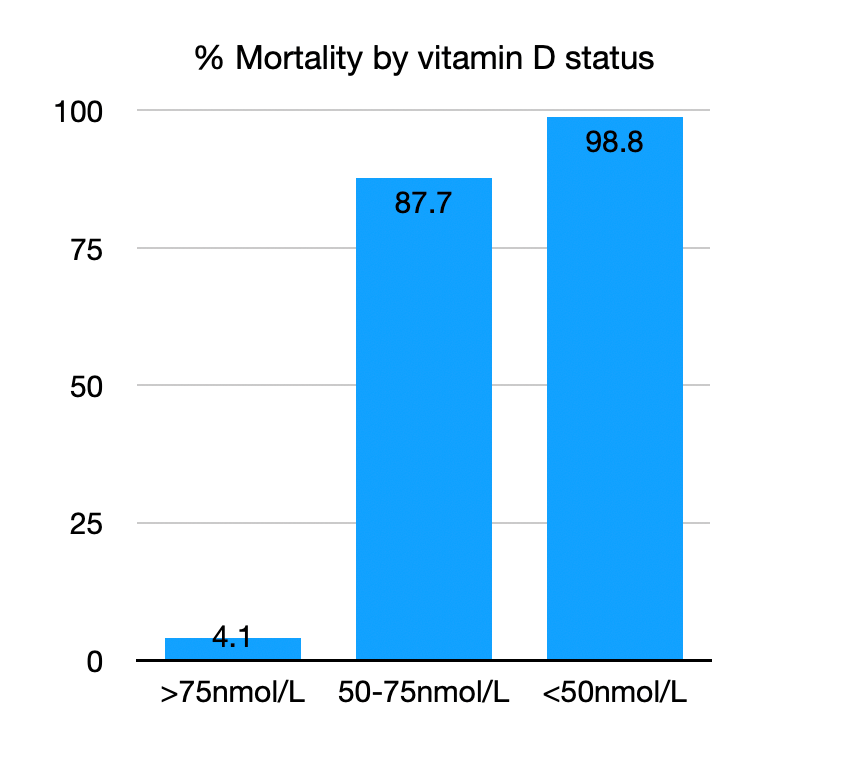 A review of data on Europe [5]For countries in Europe, the probability of developing COVID-19, and of dying from it, is negatively correlated with mean population vitamin D status, with both probabilities reaching zero above about 75nmol/L. (The chart also shows the lower vitamin D levels for the elderly in Spain and Italy. [6]) It is also known that other factors such as age, hypertension, and cardiovascular disease, obesity, and diabetes are commonly associated with death in COVID-19. [5-8] For example, the elderly population in care facilities often do not get much sunlight exposure nor adequate supplements of essential nutrients including vitamin D, which will increase their risk of serious infections. Further, the 25(OH)D level in northern European countries such as Sweden drops in late winter to ~50 nmol/L or less, which may explain their relatively high death rate from infection. [9] 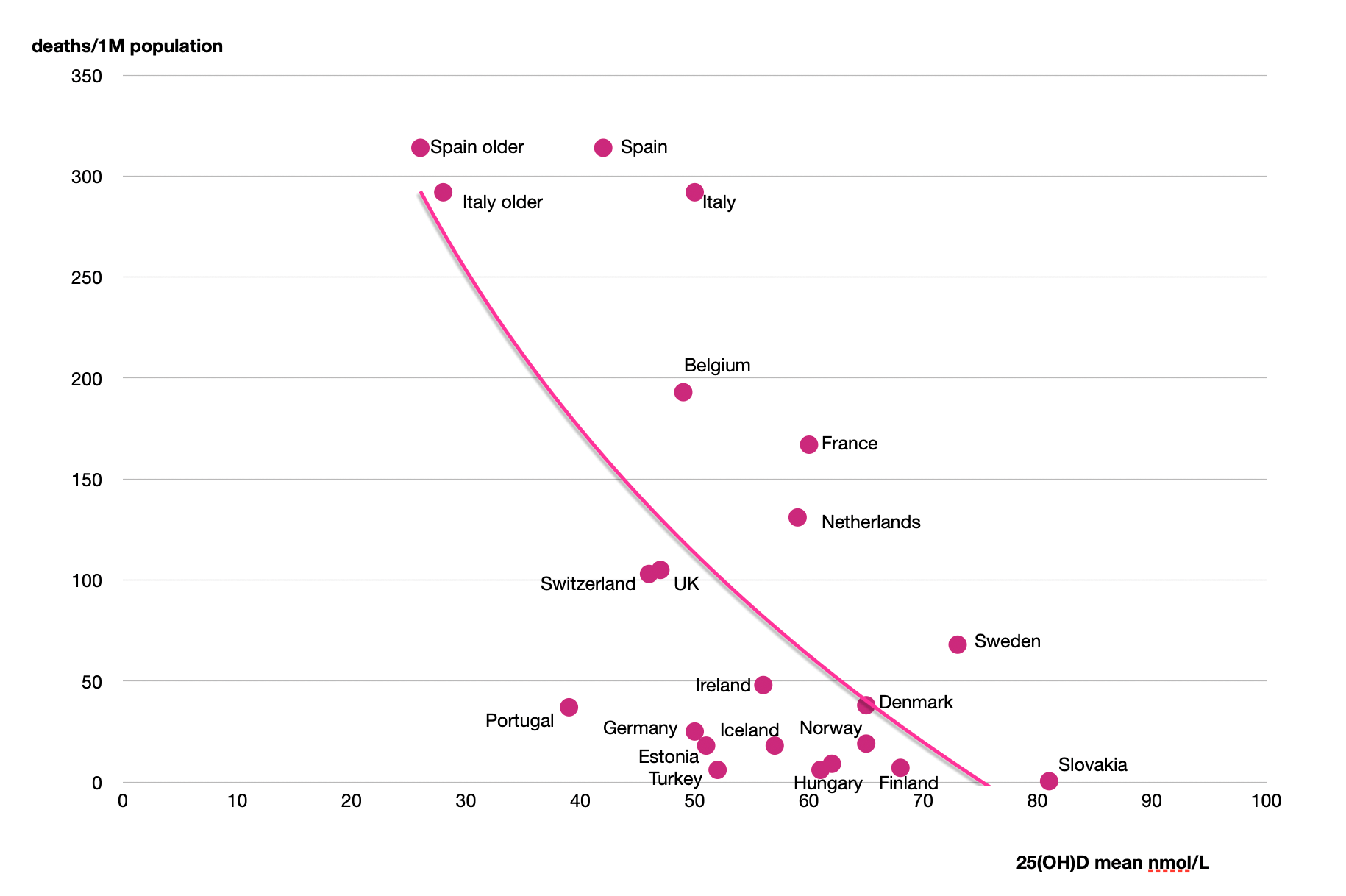 Dosage is important and generally misunderstoodRecent studies have suggested in discussion that more than 4000 IU per day of vitamin D3 may carry a risk of harm, citing the UK Scientific Advisory Committee on Nutrition report of 2016 which set the recommended Upper Level (UL) intakes of 50mcg/2000IU per day. [10] That report says; "Excessive vitamin D intakes have, however, been shown to have toxic effects (Vieth, 2006)". [10] However this is misleading, as the Vieth paper [11] states: "Published reports suggest toxicity may occur with 25(OH)D concentrations beyond 500 nmol/L." This leaves a wide margin of safety. The 3 papers mentioned above [3-5] show that a vitamin D3 blood level of at least 75 nmol/L (30 ng/ml) is needed for protection against COVID-19. Government recommendations for vitamin D intake - 400 IU/day for the UK and 600 IU/day for the USA (800 IU for >70 years) and the EU - are based primarily on bone health. This is woefully inadequate in the pandemic context. An adult will need to take 4000 IU/day of vitamin D3 for 3 months to reliably achieve a 75 nmol/L level [12]. Persons of color may need twice as much [13]. These doses can reduce the risk of infection, but are not for treatment of an acute viral infection. And since vitamin D is fat-soluble and its level in the body rises slowly, for those with a deficiency, taking a initial dose of 5-fold the normal dose (20,000 IU/day) for 2 weeks can help to raise the level up to an adequate level to lower infection risk. Other essential nutrients can helpAs mentioned above, many studies have shown that for those deficient in essential nutrients, a protocol that includes vitamin D, vitamin C, magnesium, and zinc can decrease the risk of infection for viruses, including those similar to COVID-19.[1] Recommended preventive adult doses are vitamin C, 3000 mg/day (in divided doses, to bowel tolerance), magnesium, 400 mg (in malate, citrate, or chloride form), zinc, 20 mg. [1] References1. Saul AW. (2020) Vitamin C Protects Against Coronavirus. Orthomolecular Medicine News Service http://orthomolecular.org/resources/omns/v16n04.shtml 2. Downing D. (1988) Day Light Robbery. Arrow Books, London. ISBN-13: 978-0099567400 3. Alipio MM. (2020) Vitamin D supplementation could possibly improve clinical outcomes of patients infected with Coronavirus-2019 (COVID- 2019). Preprint available at SSRN: https://ssrn.com/abstract=3571484 4. Raharusuna P, Priambada S, Budiarti C et al. (2020) Patterns of COVID-19 Mortality and Vitamin D: An Indonesian Study. 5. Ilie, P., Stefanescu, S., Smith, L. (2020) The role of Vitamin D in the prevention of Coronavirus Disease 2019 infection and mortality. Research Square preprint. https://europepmc.org/article/ppr/ppr147305 6. Lips P, Cashman K, Lamberg-Allardt C et al (2019) Current vitamin D status in European and Middle East countries and strategies to prevent vitamin D deficiency: a position statement of the European Calcified Tissue Society. Eur J Endocrinol. 180:23-54. https://europepmc.org/article/MED/30721133 7. Oaklander M (2020) Almost Every Hospitalized Coronavirus Patient Has Another Underlying Health Issue, According to a Study of New York Patients. Time Magazine, April 22, 2020. https://time.com/5825485/coronavirus-risk-factors 8. Richardson S, Hirsch JS, Narasimhan M. (2020) Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA. 323:2052-2059. https://jamanetwork.com/journals/jama/fullarticle/2765184 9. Klingberg E, Oleröd G, Konar J, et al. (2015) Seasonal variations in serum 25-hydroxy vitamin D levels in a Swedish cohort. Endocrine, 49:800-808. https://pubmed.ncbi.nlm.nih.gov/25681052 10. UK Scientific Advisory Committee on Nutrition (SACN) (2016) Vitamin D and Health. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/537616/SACN_Vitamin_D_and_Health_report.pdf 11. Vieth R (2006) Critique of the considerations for establishing the tolerable upper intake level for vitamin D: critical need for revision upwards. J Nutr, 136:1117-1122. https://pubmed.ncbi.nlm.nih.gov/16549491 12. Vieth R, Chan PC, MacFarlane GD. (2001) Efficacy and safety of vitamin D(3) intake exceeding the lowest observed adverse effect level. Am J Clin Nutr, 73:288-294. https://pubmed.ncbi.nlm.nih.gov/11157326 13. Cashman KD, Ritz C, Adebayo FA, et al. (2019) Differences in the dietary requirement for vitamin D among Caucasian and East African women at Northern latitude. Eur J Nutr. 58:2281-2291. https://pubmed.ncbi.nlm.nih.gov/30022296 Nutritional Medicine is Orthomolecular MedicineOrthomolecular medicine uses safe, effective nutritional therapy to fight illness. For more information: http://www.orthomolecular.org Find a DoctorTo locate an orthomolecular physician near you: http://orthomolecular.org/resources/omns/v06n09.shtml The peer-reviewed Orthomolecular Medicine News Service is a non-profit and non-commercial informational resource. Editorial Review Board:Vladimir Arianoff, M.D. (Belgium) Andrew W. Saul, Ph.D. (USA), Editor-In-Chief Comments and media contact: drsaul@doctoryourself.com OMNS welcomes but is unable to respond to individual reader emails. Reader comments become the property of OMNS and may or may not be used for publication. Click here to see a web copy of this news release: https://orthomolecular.acemlna.com/p_v.php?l=1&c=160&m=164&s=b5a4d78a62acf8d7d34cf4c3d0c1905f |
|
|
This news release was sent to dennis_mangan@hotmail.com. If you no longer wish to receive news releases, please reply to this message with "Unsubscribe" in the subject line or simply click on the following link: unsubscribe . To update your profile settings click here . This article may be reprinted free of charge provided 1) that there is clear attribution to the Orthomolecular Medicine News Service, and 2) that both the OMNS free subscription link http://orthomolecular.org/subscribe.html and also the OMNS archive link http://orthomolecular.org/resources/omns/index.shtml are included.
|
|